 By Dr. Shantanu Mallick MBBS (Cal), DA (Mum), FIPP (UK)
By Dr. Shantanu Mallick MBBS (Cal), DA (Mum), FIPP (UK)
Pain Physician, Pain Care Clinic (Seawoods west)
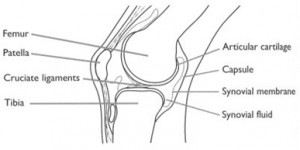
The largest joint in the body, the knee moves like a hinge, allowing you to sit, squat, walk or jump formed by Femur, Tibia and Patella. The ends of the bones are covered with a layer of cartilage, an elastic material that absorbs shock and allows the bones to glide easily against one another as they move. Between the tibia and femur bone there are two crescent-shaped pads of connective tissue (meniscus) that reduce friction and disperse the weight of the body across the joint. The bones are held together by a joint capsule which is supported outside by the ligaments and tendons. From cartilage breakdown, tendon injury to infections in the joint can cause painful knees.
Osteoarthritis is commonest cause of knee pain with 80% of general population by 65 yrs. of age. Exact reason is not known but stress on articular cartilage and bone leads to wear and tear to these structures. Pain around the joint increases with weight bearing and movement which improves with rest. It may be associated with morning stiffness and swelling of the joints. Clinical signs are tenderness, crepitus, joint effusion, decreased range of movement, etc. X-ray shows decreased joint space, osteophytes formation and osteoporosis of bone. Rheumatoid arthritis should be ruled out.
TREATMENT
I. NON- PHARMACOLOGICAL THERAPY: Reduction of obesity decreases load on the joints and thereby retards the disease process. Quadriceps muscle strengthening exercises improves knee pain and function. Walking stick to be held in the opposite hand of the affected joint reduces the load on the joint and is associated with decreased pain and improved function.
II.PHARMACOLOGICAL THERAPY:Paracetamol /Acetaminophen/Tramadol should be used as the first line of therapy but should not be used for prolonged period. The agents which help in regeneration are chondroitin sulphate and gulcosaminesulphate can be used.
III. INTERVENTIONS:
a. Intra-articular corticosteroid or Ozone gas injections to minimize the inflammation.
B.Intra-articular visco-supplementation with Hyaluronic acid which involves cushioning the knee joint with injections of a gel-like fluid. The fluid acts as a shock absorber and enables the bones to move more smoothly.
c. Platelet Rich Plasma therapy or PRP therapy:A new treatment that is being studied in different part of the world extensively. PRP or “Platelet Rich Plasma” is nothing but autologous (from the same person) blood with concentrations of platelets above baseline levels which also contains at least six growth factors. Normal blood contains only 6% platelets. However, in PRP, there is a concentration of 94% platelets, which translates to a powerful growth factor “cocktail” with a variety of growth factors and cytokines. This stimulates cellular proliferation and tissue regeneration which dramatically accelerate healing. (for more detail see this link http://painclinic.co.in/crps.html)
d. Surgery: Patients having very severe symptoms should be considered for surgical options like tibial osteotomy, arthroplasty and joint replacement. Surgical options should be considered, once medical line of treatment fails. Surgical options should be delayed as much because the total joint replacement might last between 10-20 years.